

Background: Richter transformation (RT) to diffuse large B-cell lymphoma (DLBCL) is a well-known complication of CLL/SLL, occurring in 2-10% of patients (pts); however, a minority transform to Hodgkin lymphoma, termed Hodgkin variant of RT (HvRT). Because of the rarity of HvRT, there is limited information regarding prognostic factors and treatment approach. The aim of this study was to evaluate clinical characteristics, treatment and survival of HvRT in a population based cohort of CLL/SLL pts in BC.
Methods: Provincial databases were retrospectively reviewed from Jan. 1994 - Feb. 2020 to identify all CLL/SLL pts in BC with histologically proven HvRT using central pathology review. Overall survival (OS) was defined from HL diagnosis to death/last follow-up (f/u); progression-free survival (PFS) was defined from HL diagnosis to lymphoma progression, death or last f/u.
Results: 32 pts with HvRT from CLL (N=18) or SLL (N=14) were identified. Median f/u for living pts from CLL/SLL diagnosis was 129 months (mos) (range, 25-504). Most pts were male (87%) with median age at CLL/SLL and HL diagnoses of 64 years (y) (range, 35-83) and 71 y (range, 51-86), respectively. Median interval from CLL/SLL diagnosis to HvRT was 67 mos (range, 0-403), with composite CLL/SLL and HL diagnosed in 5 pts (16%). At CLL/SLL diagnosis, 50% (15/30) had Rai or Ann Arbor stage 3-4; 7% (1/14) had del(17p), 29% (4/14) del(13q), 0% (0/14) del(11q), 29% (4/14) trisomy 12 and 50% (7/14) had no abnormalities. Most pts (80%; 24/30) had treatment for CLL/SLL prior to HvRT: purine analogues (PA) in 67% (20/30), alkylators in 50% (15/30), rituximab in 60% (18/30) and ibrutinib in 17% (5/30%). Median number of treatment lines prior to HvRT was 2 (range, 0-4) and median time from last CLL/SLL therapy to HvRT was 15 mos (range, 1-107).
HvRT was characterized by Ann Arbor stage 3-4 in 87% (25/29) of cases, B symptoms in 67% (18/27), International Prognostic Score (IPS) ≥ 4 in 67% (18/27), and Epstein Barr virus (EBV) positivity in 59% (13/22). Richter Prognosis Score (RPS) was low risk (RPS 0-1) in 48% (10/21 pts), low-intermediate (RPS 2) in 33% (7/21) and high-int/high (RPS 3-5) in 19% (4/21). ABVD (adriamycin, bleomycin, vinblastine and dacarbazine) or ABVD-like therapy (AVD or modified ABVD dose/regimen) was the most common primary HL therapy, used in 65% (20/31). Others were alkylator-based regimens in 13% (4/31); brentuximab, ibrutinib and cyclosporine in 1 case each, and local excision in 1 case. 4 pts had radiotherapy for primary (N=2) or relapsed HL (N=2). No pts had autologous stem cell transplant (SCT); however, 1 had a reduced intensity allogeneic SCT 10.8 mos after HvRT. 3 pts (10%) had no HL therapy due to frailty. Median f/u for living pts from HvRT was 25 mos (range, 4-100). 18 pts (56%) experienced lymphoma progression: 5 CLL/SLL, 8 HL, 1 with a second RT to DLBCL and 4 with unknown subtype. One pt, who first progressed with CLL after HvRT, subsequently developed a second RT to DLBCL.
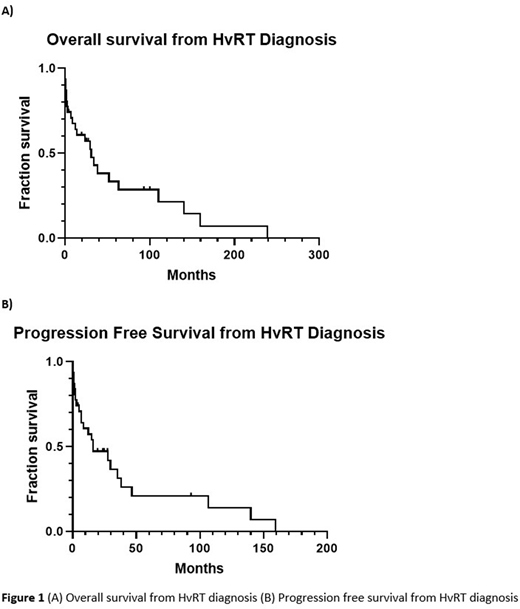
At time of last f/u, 75% of pts (24/32) died. Cause of death was lymphoma in 14 pts (3 CLL/SLL; 7 HL; 2 DLBCL; 2 unknown subtype), treatment-related toxicity in 5, secondary malignancy in 2, other causes in 2 and unknown cause in 1. The 2 y OS and PFS from HvRT were 55% (95% CI: 36-71%) and 46% (95% CI: 28-62%), respectively, Fig. 1A-B. Factors at HvRT significantly affecting OS included low hemoglobin (< 120 vs ≥ 120 x 109/L, P=.02), elevated lactate dehydrogenase (elevated vs normal, P=.04), high IPS (IPS ≥ 4 vs < 4, P=.04), and, among pts who received chemotherapy (N=27), primary HL therapy (non-ABVD vs ABVD/ABVD-like, P=.048). The only factor significantly associated with PFS was primary HL treatment (P<.001). 2 y OS and PFS for those who received ABVD/ABVD-like regimens (N=20) were 74% (95% CI: 49-89%) and 70% (95% CI: 45-85%), respectively. Time from last CLL therapy to HvRT (≤ 12 vs >12 mos, P=.72), prior treatment for CLL (P=0.15), prior PA therapy (P=.14), B symptoms at HvRT (P=0.12), EBV positivity (P=.24) and RPS (0-2 vs 3-5, P=.85) did not significantly impact OS or PFS.
Conclusion: In this real-world population-based cohort of CLL/SLL pts, HvRT was associated with poor clinical outcomes, with a median OS less than 3 y from time of HvRT. This may be in part due to the older age of HvRT diagnosis, which limits the ability to give curative therapy with ABVD. Further biological and clinical investigation of this rare entity, particularly in the era of novel agents, is warranted to improve outcomes.
Villa:Celgene: Consultancy, Honoraria; Janssen: Consultancy, Honoraria; Roche: Consultancy, Honoraria, Research Funding; AZ: Consultancy, Honoraria, Research Funding; Kite/Gilead: Consultancy, Honoraria; Nano String: Consultancy, Honoraria; Seattle Genetics: Consultancy, Honoraria; Sandoz Canada: Consultancy, Honoraria; Immunovaccine: Consultancy, Honoraria; Purdue Pharma: Consultancy, Honoraria. Scott:NIH: Consultancy, Other: Co-inventor on a patent related to the MCL35 assay filed at the National Institutes of Health, United States of America.; Roche/Genentech: Research Funding; Abbvie: Consultancy; AstraZeneca: Consultancy; Janssen: Consultancy, Research Funding; NanoString: Patents & Royalties: Named inventor on a patent licensed to NanoString, Research Funding; Celgene: Consultancy. Sehn:Takeda: Consultancy, Honoraria; F. Hoffmann-La Roche Ltd: Consultancy, Honoraria, Research Funding; MorphoSys: Consultancy, Honoraria; Merck: Consultancy, Honoraria; Lundbeck: Consultancy, Honoraria; Karyopharm: Consultancy, Honoraria; Gilead: Consultancy, Honoraria; Kite: Consultancy, Honoraria; Janssen: Consultancy, Honoraria; Celgene: Consultancy, Honoraria; Acerta: Consultancy, Honoraria; Genentech, Inc.: Consultancy, Honoraria, Research Funding; AstraZeneca: Consultancy, Honoraria; Apobiologix: Consultancy, Honoraria; Seattle Genetics: Consultancy, Honoraria; Servier: Consultancy, Honoraria; TG therapeutics: Consultancy, Honoraria; Chugai: Consultancy, Honoraria; Verastem Oncology: Consultancy, Honoraria; Teva: Consultancy, Honoraria, Research Funding; AbbVie: Consultancy, Honoraria; Amgen: Consultancy, Honoraria. Connors:Seattle Genetics: Other: Sponsorship to educational presentations; Takeda: Other: Sponsorship to educational presentations. Toze:Janssen: Consultancy. Savage:Merck, BMS, Seattle Genetics, Gilead, AstraZeneca, AbbVie, Servier: Consultancy; BeiGene: Other: Steering Committee; Merck, BMS, Seattle Genetics, Gilead, AstraZeneca, AbbVie: Honoraria; Roche (institutional): Research Funding. Gerrie:Roche: Research Funding; Sandoz: Consultancy; Astrazeneca: Consultancy, Research Funding; AbbVie: Consultancy, Honoraria, Research Funding; Janssen: Consultancy, Honoraria, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal